Overview

Fallen arches, also called flat feet or pes planus, is a condition in which the entire bottom of the foot touches the ground when a person is standing. A normal foot has an arch between the heel and the ball of the foot. Fallen arches are typically an acquired condition, though flat feet may be present from childhood if the arch never developed in the first place. In some cases, usually those in which the arch never developed, flat feet are not a cause for concern. If they develop in adulthood, however, causing a rigid flat foot, the condition is usually accompanied by pain and can cause serious health issues.
Causes
When flat feet develop at a later age, they are known as fallen arches. The arches may fall because the muscles supporting them are no longer able to do so. In addition the spring ligament within the foot may have lost some of its tension allowing the arch of the foot to flatten. Other conditions causing fallen arches include sudden weight gain, a nervous system injury, or a loss of sensation caused by a disease such as diabetes. Most people with fallen arches are flat on both feet.
Symptoms
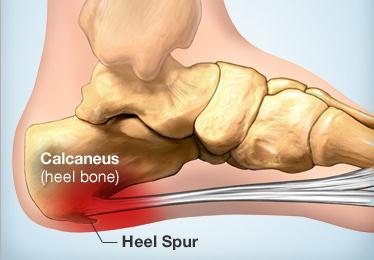
The primary symptom of fallen arches is painful or achy feet in the area in which the foot arches or on the heel. This area may become swollen and painful to stand still on. This causes the patient to improperly balance on their feet which in turn will cause other biomechanical injuries such as back, leg and knee pain.
Diagnosis
You can test yourself to see if you have flat feet or fallen arches by using a simple home experiment. First, dip your feet in water. Then step on a hard flat surface, like a dry floor or a piece of paper on the floor, where your footprints will show. Step away and examine your foot prints. If you see complete/full imprints of your feet on the floor, you may have fallen arches. However, it?s important to seek a second option from a podiatrist if you suspect you have fallen arches so they can properly diagnose and treat you.
fallen arches insoles
Non Surgical Treatment
Fallen arches lead to flat feet, where the arch of your foot collapses and may even touch the ground. This condition is common in infants and young children because your arches are still developing during childhood, says the Instep Foot Clinic. If your flat feet persist into adulthood, or the condition causes pain, a doctor or podiatrist may prescribe strengthening exercises as part of your treatment.
Surgical Treatment

Fallen arches may occur with deformities of the foot bones. Tarsal coalition is a congenital condition in which the bones of the foot do not separate from one another during development in the womb. A child with tarsal coalition exhibits a rigid flat foot, which can be painful, notes the patient information website eOrthopod. Surgery may prove necessary to separate the bones. Other foot and ankle conditions that cause fallen arches may also require surgery if noninvasive treatments fail to alleviate pain and restore normal function.
Fallen arches, also called flat feet or pes planus, is a condition in which the entire bottom of the foot touches the ground when a person is standing. A normal foot has an arch between the heel and the ball of the foot. Fallen arches are typically an acquired condition, though flat feet may be present from childhood if the arch never developed in the first place. In some cases, usually those in which the arch never developed, flat feet are not a cause for concern. If they develop in adulthood, however, causing a rigid flat foot, the condition is usually accompanied by pain and can cause serious health issues.
Causes
When flat feet develop at a later age, they are known as fallen arches. The arches may fall because the muscles supporting them are no longer able to do so. In addition the spring ligament within the foot may have lost some of its tension allowing the arch of the foot to flatten. Other conditions causing fallen arches include sudden weight gain, a nervous system injury, or a loss of sensation caused by a disease such as diabetes. Most people with fallen arches are flat on both feet.
Symptoms
The primary symptom of fallen arches is painful or achy feet in the area in which the foot arches or on the heel. This area may become swollen and painful to stand still on. This causes the patient to improperly balance on their feet which in turn will cause other biomechanical injuries such as back, leg and knee pain.
Diagnosis
You can test yourself to see if you have flat feet or fallen arches by using a simple home experiment. First, dip your feet in water. Then step on a hard flat surface, like a dry floor or a piece of paper on the floor, where your footprints will show. Step away and examine your foot prints. If you see complete/full imprints of your feet on the floor, you may have fallen arches. However, it?s important to seek a second option from a podiatrist if you suspect you have fallen arches so they can properly diagnose and treat you.
fallen arches insoles
Non Surgical Treatment
Fallen arches lead to flat feet, where the arch of your foot collapses and may even touch the ground. This condition is common in infants and young children because your arches are still developing during childhood, says the Instep Foot Clinic. If your flat feet persist into adulthood, or the condition causes pain, a doctor or podiatrist may prescribe strengthening exercises as part of your treatment.
Surgical Treatment
Fallen arches may occur with deformities of the foot bones. Tarsal coalition is a congenital condition in which the bones of the foot do not separate from one another during development in the womb. A child with tarsal coalition exhibits a rigid flat foot, which can be painful, notes the patient information website eOrthopod. Surgery may prove necessary to separate the bones. Other foot and ankle conditions that cause fallen arches may also require surgery if noninvasive treatments fail to alleviate pain and restore normal function.



 Morton's neuroma is a swollen, inflamed nerve in the foot.Morton's neuroma causes a "burning" sharp pain on the bottom of the foot. Treatments for Morton's neuroma include resting the foot, better-fitting shoes, anti-inflammation medications, ice packs, and operation. A neuroma is growth (benign tumor) that arises in nerve cells. A Morton's neuroma is a swollen, inflamed nerve located between the bones at the ball of the foot. The most common location of a Morton's neuroma is in either the second or the third spacing from the base of the big toe.
Morton's neuroma is a swollen, inflamed nerve in the foot.Morton's neuroma causes a "burning" sharp pain on the bottom of the foot. Treatments for Morton's neuroma include resting the foot, better-fitting shoes, anti-inflammation medications, ice packs, and operation. A neuroma is growth (benign tumor) that arises in nerve cells. A Morton's neuroma is a swollen, inflamed nerve located between the bones at the ball of the foot. The most common location of a Morton's neuroma is in either the second or the third spacing from the base of the big toe.
 Overview
Overview
 When the big toe is misaligned, it creates an unnatural bump on the inside of the forefoot (see image below). In addition to being unsightly, the lump or bunion can cause pain and make buying shoes difficult. Some people are born predisposed to bunions. But most people acquire them over time from ill-fitting footwear that squeezes the big toe inward toward the other toes. About four out of five bunion pain patients are female, a near perfect fit for the bad shoe theory. The good news, Bunions can be corrected, often with better-fitting shoes and custom orthotics. There are also some cases that cause severe bunion pain and do not respond to conservative treatment. For those patients, bunion surgery called bunionectomy may be necessary.
When the big toe is misaligned, it creates an unnatural bump on the inside of the forefoot (see image below). In addition to being unsightly, the lump or bunion can cause pain and make buying shoes difficult. Some people are born predisposed to bunions. But most people acquire them over time from ill-fitting footwear that squeezes the big toe inward toward the other toes. About four out of five bunion pain patients are female, a near perfect fit for the bad shoe theory. The good news, Bunions can be corrected, often with better-fitting shoes and custom orthotics. There are also some cases that cause severe bunion pain and do not respond to conservative treatment. For those patients, bunion surgery called bunionectomy may be necessary.


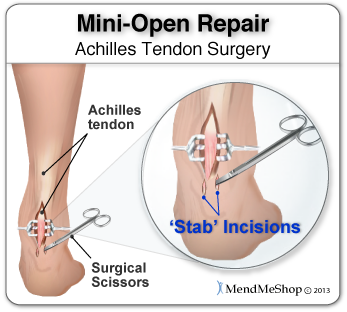 The Achilles tendon runs from the calf muscles at the back of the lower leg and inserts at the back of the heel. A torn achilles can be a partial rupture or a total rupture. A total rupture is more common in men affecting them 10 times more than women. Injury typically occurs 30 to 40 minutes into a period of exercise rather than at the start of a session and nearly always happens from a sudden explosive movement or bending the foot upwards. Many patients are able to continue to function following an achilles rupture due to other muscles compensating although the injured leg will be significantly weaker. There are four key tests which can help diagnose a ruptured achilles tendon.
The Achilles tendon runs from the calf muscles at the back of the lower leg and inserts at the back of the heel. A torn achilles can be a partial rupture or a total rupture. A total rupture is more common in men affecting them 10 times more than women. Injury typically occurs 30 to 40 minutes into a period of exercise rather than at the start of a session and nearly always happens from a sudden explosive movement or bending the foot upwards. Many patients are able to continue to function following an achilles rupture due to other muscles compensating although the injured leg will be significantly weaker. There are four key tests which can help diagnose a ruptured achilles tendon.


